


DoD's Mismanaged Biodefense Program
Does anyone care?

I do want to talk about the U.S. nuclear modernization program, it’s a much more interesting topic that engages the national security community. But I want to take advantage of the recent release of this DoD article trumpeting the release of funds from the DoD Chemical and Biological Defense Program (CBDP) to DOE’s Lawrence Livermore National Laboratory (LLNL) for the purposes of using a supercomputer “to develop new biodefense capabilities for national security purposes.” This builds from an agreement between DoD and DOE/NNSA “to work together on the nation’s toughest biodefense challenges.”
So let that sink in for a second. These defense funds are not going to improve the military’s biodefense capabilities, which are, to say the least, lacking. No, the OSD acquisition leaders have decided that there are national priorities for biodefense that supersede the military’s needs and requirements, because COVID demonstrated that the Department of Health and Human Services (HHS) has issues. You can read the justification for this policy direction in the 2023 Biodefense Posture Review. For the record, I saw the sausage being made for the Biodefense Posture Review and I thought it was an incredibly poor piece of work. But I’m not going to talk about the BPR today. I want to use the policy model that I discussed in the previous post as a way to identify the significant management problems in the DoD’s CBDP, specifically in the area of biological defense. Beware, it’s a scary topic, especially post-COVID.
I jest. This overly busy chart displays the usual trope of distorted information about biotechnology that has gone on since the 1970s, that the misuse of the “life sciences” will result in nefarious actors creating new biological weapons. Hasn’t happened yet, but it’s an old trope for this community seeking to influence policymakers and budget managers (who often lack a scientific background) to provide more funds to their research area. It hasn’t been entirely successful in achieving this goal but people keep using this because it looks sexy. The latest scare is how terrorists are going to use artificial intelligence to make bioweapons. There’s no actual basis to these statements but why let facts get in the way of a good story.
Military biodefense has a checkered past. In 1990, going into the Persian Gulf, there were for all intents and purposes no biological detectors and no FDA-approved vaccines for biowarfare agents. The protective suits, collective protection, and decon systems worked but only if you knew that a biological agent was used. This failure was largely because the Army medical community made a conscious decision to focus its research for medical countermeasures on naturally-occurring diseases that were impacting soldiers’ health as opposed to biological weapons that hadn’t been used throughout the Cold War. In 2003, this deficiency was somewhat improved by putting laboratories on HMMWVs and we had anthrax and smallpox vaccines. The military played around with a biological-only defense concept but it went nowhere. That was it. It hasn’t really improved since. Work on improving biodefense was slow and costly. COVID-19 created a situation where HHS needed the CBDP to act as a vehicle for moving funds for its vaccine candidates. Now the CBDP wants to work in the health care business instead of the military biodefense business.
We can use the Jones’ model for public policy to study the players who work biodefense (and CBRN defense in general) acquisition to better understand this issue. This process has policymakers working with technical agencies, executing programs funded by Congress, and criticism from reformist groups. Policymakers are supposed to use a rational approach to identifying problems and defining policy objectives that can be solved with a deliberate and focused approach. They can fail by not considering the institutional and political challenges of a policy issue. Within biodefense, the OSD acquisition leaders would say that the policy objectives are clear - to address all biological threats, irrespective of their origin, to protect the nation and the warfighter. But that’s not really a clear or achievable goal, nor should acquisition leaders be forming these policy objectives.
The military services have the responsibility to protect their troops from adversaries using biological weapons. We call this “CBRN defense,” which develops non-medical and medical defense gear used during warfighting scenarios. At the same time, the services have to protect their forces from infectious and non-communicable diseases, especially given the foreign climates in which they may operate. This second function falls under force health protection. And the military has a few BSL-3/4 labs that require strict biosecurity/biosafety regulations based on CDC guidance. These are different but related areas of expertise that require distinct execution roles. What we’re arguing about is who should execute these roles and who should pay for them.
There are multiple agencies within DoD who address “biological threats” as defined by the Biodefense Posture Review. OSD policy offices are supposed to provide advice that turns into strategies and policy objectives. The ASD for Space Policy oversees countering WMD policy (which includes military biodefense) as well as nuclear strategy. The ASD for SO/LIC leads the DoD response to emerging health crises overseas such as the Ebola outbreak in West Africa. ASD for Homeland Defense provides guidance on pandemic outbreaks on U.S.-based military installations. The ASD for Health Affairs oversees … wait for it … military health and force health protection policies, which includes the threat of natural disease outbreaks. The ASD for Nuclear, Chemical and Biological Defense (NCB) oversees the research and development of military biodefense equipment intended to counter adversarial use of biological weapons. All ASD NCB is supposed to do is to ensure that the CBDP is run efficiently as an acquisition program and that the annual CBDP budget proposal is rolled up into the OSD POM. That’s all. But instead of OSD policy or OSD personnel and readiness leading the discussion on DoD’s policy objectives addressing “biological threats,” the DoD has OSD acquisition leaders heading the new Biodefense Council to coordinate its biodefense efforts.
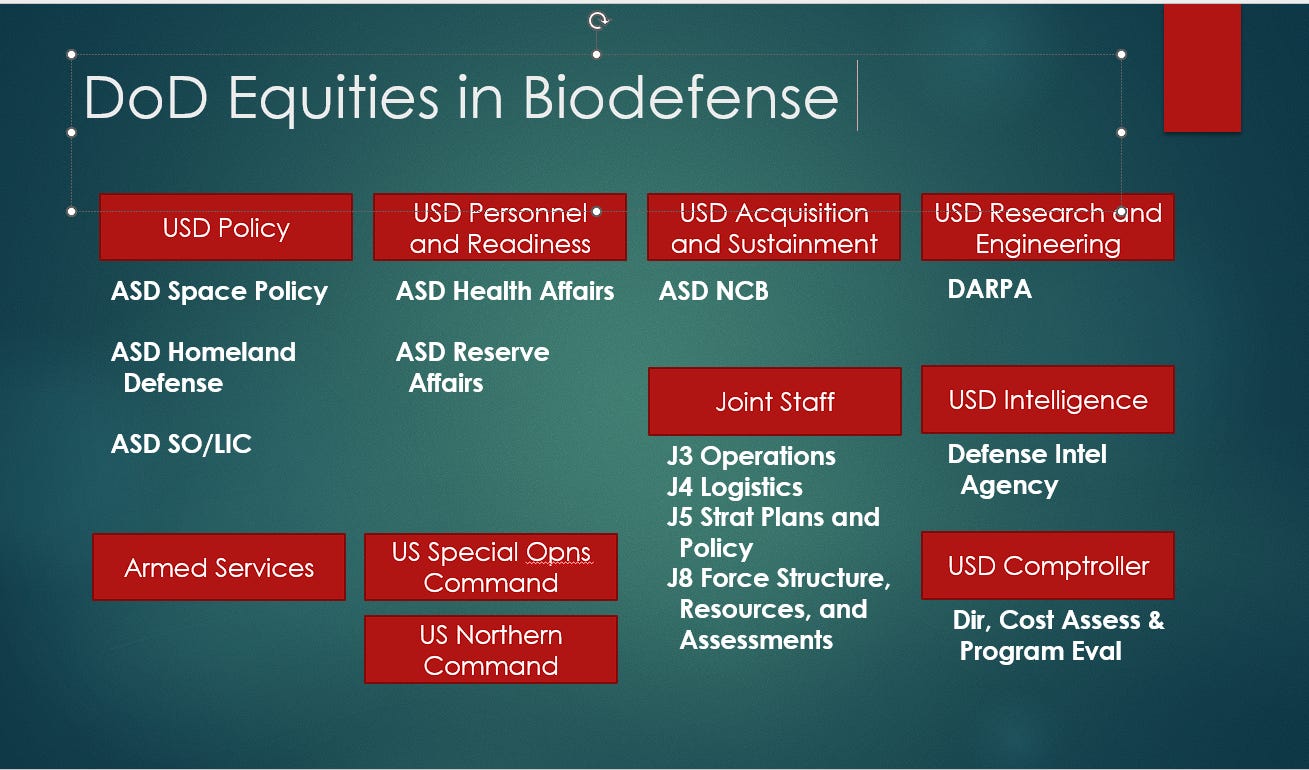
My opinion only, the counter-WMD office under ASD Space Policy doesn’t counter what they know is not just bad policy but also inappropriate conduct for the acquisition community because they eschew intra-department conflict. ASD NCB has the money, the clout, and the influence to throw their weight around and so Policy just stays quiet rather than to tell their acquisition colleagues to limit their scope to acquisition issues. ASD Health Affairs doesn’t care if the CBDP spends its money on natural disease outbreaks because it complements the Defense Health Agency portfolio, and Health Affairs can ignore ASD NCB on issues relating to its much, much larger force health protection budget. DARPA’s biodefense funds are similarly firewalled off from ASD NCB control. The Joint Staff is, well, the Joint Staff. They never push back against OSD civilians, that would be impolite (and politically dangerous). The combatant commands outside of SOCOM and NORTHCOM do not weigh in here. Too many other priorities take precedent.
The armed services and the Defense Threat Reduction Agency (DTRA) represent the technical branch of policy processes. They are specialists whose problems are defined by other offices and they implement policy initiatives as directed. Technicians can get in trouble when they are called upon to expand upon policy issues, because they are limited by their training and experience that doesn’t include engaging in broad policy debates. The armed services have the responsibility to organize, train, and equip their personnel as they see fit, given White House and OSD direction. The armed services own the laboratories that research and develop the chemical-biological defense gear that is funded and overseen by the CBDP and they have to spend operations and maintenance funds to maintain the gear. We know that the CBDP was designed to address service requirements, because Congress said so when it created the CBDP in the mid-1990s to address shortfalls in service readiness following the 1991 Persian Gulf War. We can examine strategic missions and goals, which creates “silos of excellence” regarding biological threats in this figure.
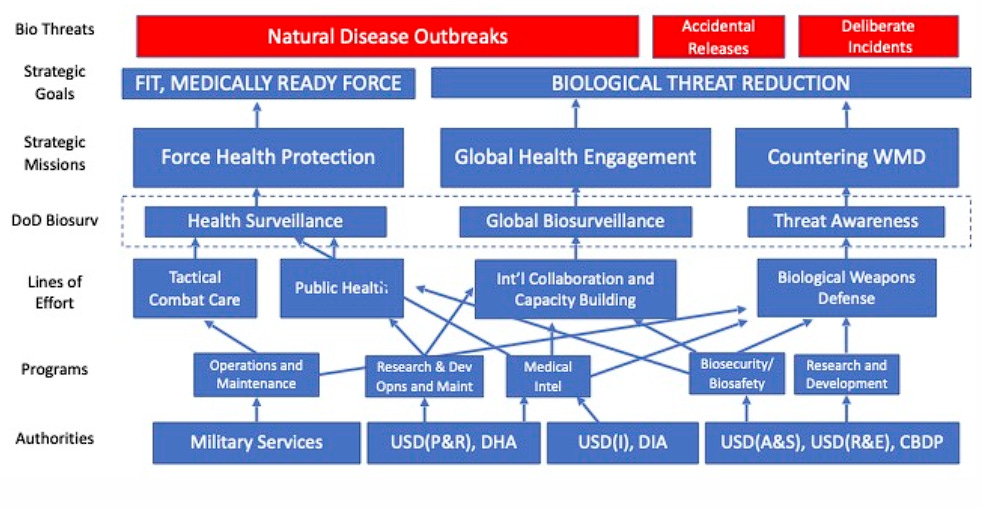
This figure demonstrates two things, first that it is impossible to put all biodefense programs and initiatives into one business area as the OSD acquisition office wants to do. Second, it demonstrates whose funds are going to what policy initiatives. The service leaders ultimately care about what comes out of their budgets, and that’s force health protection programs. They understand the need for CBRN defense gear but U.S. forces haven’t been threatened by chem-bio weapons since 1990. They don’t particularly care about how well the CBDP runs or what direction OSD acquisition wants it to go because it isn’t their money. The Army does have a “DoD Executive Agent” role for CB defense research and development that is intended to both champion all of the services’ requirements and approve the CBDP annual budget. In general, it fails to perform this role and so OSD acquisition set up a “governance framework” to run the program for them. This isn’t appropriate for an oversight role but there’s no will to push back against OSD civilians with a determined agenda.
In theory, the services could object to the CBDP’s misuse of funds and appeal to the Joint Requirements Oversight Council. They don’t because chem-bio defense is not important enough to their day-to-day missions. Inside the Beltway, there are no general officers who champion this issue, and the colonels who are involved don’t want to fight the system. They only have a few years to spend in the Beltway and then they get to return to the field and continue their careers. Why ruin that experience by jousting with some political appointee over poor acquisition decisions?
Then there’s Congress. There are many, many subcommittees that oversee health care issues, too many to list here (I talk about them in my book “BIOCRISIS”). Every natural disease and non-communicable disease has an advocacy group that engages Congress and HHS on its particular concern. There’s one subcommittee in the House and one in the Senate that address WMD-related issues. Once a year, the ASD Space, ASD NCB, DTRA director, and U.S. Special Operations Command brief these two subcommittees on their activities and thank Congress for continuing to fund their programs. Congress listens to the testimonies and then decides that additional funds for countering WMD or CBRN defense is unnecessary. It’s a very polite and routine process. Congress does not ask the Army, Navy, Air Force, or Marine Corps leadership as to the adequacy of their biodefense capabilities, nor does that service leadership ever mention biodefense or countering WMD in annual posture statements. There are always other priorities.
In a 2023 brief to the House subcommittee on Intelligence and Special Operations, the Honorable Deborah Rosenblum stressed the need to change its acquisition strategy and to prepare for “a broad spectrum of biological threats, whether naturally occurring, accidental, or deliberate.” No one questioned this as an inappropriate goal in a WMD strategy. The Honorable John Plumb highlighted the need to get $630 million to U.S. European Command to procure CBRN defense equipment - because for some reason, the services who are supposed to outfit their forces in Europe were not providing that capability? Not sure that point was well-thought out, and I’m not sure if the funding was ever provided. There were other topics addressed - the Cooperative Threat Reduction program, the chemical demilitarization program, the SLBM-N proposal - and this is a good opportunity for the congresspeople to get some up-to-date information - but in general, Congress doesn’t care about CB defense to the extent of 1) wanting to provide more funding so as to address identified, critical capability gaps, or 2) understanding the difference between DoD funds for countering biological weapons and DoD funds for protecting against natural disease outbreaks.

The last group of policy influencers are the reformists, the critics of government programs to include think tanks and advocacy groups who want to influence the policymakers, the services, and Congress to spend funds in the direction that they feel is appropriate. Very often, the reformists and activists have a vision on where public policy should go, a vision that is not constrained by government funding, organizational authorities, or the tyranny of time. This is not to say that they are irrational, far from it. They are coldly logical and have their selectively-developed points lined up in a way that drives their preferred agenda as a desired outcome. If you want data on a particular technical niche topic, you go to the think tanks and advocacy groups. Even if no one in the executive branch of government is listening, Congress will give them an ear, because it’s often data that can be used toward a legislator’s particular interest or for a good witness presentation at a hearing.
There aren’t many reformists who work military biodefense topics. After the Amerithrax incident in 2001, there was a flurry of work on bioweapons in the think tanks but that hasn’t happened in the past 10-15 years. WMD work is focused solely on nuclear weapons, and the arms control think tanks don’t have much to do with chemical or biological warfare outside of the CWC and BWC review conferences. There are lots of think tanks that do global health issues but that’s not the same as military biodefense. There are two industry groups, a CBRN Defense Division in the National Defense Industrial Assocation and the CBRNE Industry Group. If you drew a Venn diagram of these two groups, it would closely resemble a single circle. They don’t do policy, they just watch where the budget goes.
The Bipartisan Commission on Biodefense is the most active voice in this area, and they’re largely funded by pharmaceutical firms. They consistently warn that the U.S. is “dangerously unprepared for outbreaks and biological attacks” and have offered many recommendations on how to fix this situation. Practically none of their recommendations have been undertaken, because they are not executable, but the Commission gets a lot of press. They approved the CBDP’s funding a DOE/LLNL supercomputer initiative, which locks into my mind that this initiative is no good. I have no use for the Commission or their reports.
We actually have no idea what (another) model or simulation of natural disease outbreaks or how this model’s assumptions will be developed to be useful in developing new biodefense capabilities. Meanwhile, the CBDP is not delivering new biological detectors, is stalled on developing new protective suits to replace the decades-old JSLIST, has few to no significant decon capabilities for biologically-contaminated buildings and large-frame aircraft, and doesn’t have the funds for new vaccines for known biological warfare agents or medical countermeasures for radiological exposure. But please, do go on about “gamechangers.”
Dr. Asha George, executive director of the Bipartisan Commission, said in October 2021, “We cannot regulate national security issues to healthcare and public health institutions that have a whole lot of things to address, not just [naturally-occurring diseases]. And who do not have the resources or capability or capacities necessary to fight a national security threat all by themselves.” This is dangerously foolish language. HHS has the direct mandate to address global health challenges and pandemics with a huge budget and personnel to execute that mission. DoD’s research and development funding is a drop in the ocean in comparison. But as Dan Drezner pointed out recently, everything is national security now because everyone is fighting for more federal resources. Why would anyone offer a rational review of any significant challenge when one could just trot out jingoistic narratives like this?
I don’t believe the Bipartisan Biodefense Commission is particularly effective in moving the needle in any direction, nor are the two industry groups who frankly don’t particularly care what the policy narrative is as long as the funds flow. Nothing in defense policy or health care policy is really changing as a result of its efforts. But it does confuse the issues by allowing a false narrative to be circulated without any serious examination by others. And meanwhile the national security community ignores this debate because science is hard and conventional and nuclear threats are so much more interesting.
I worked for and with the CBDP for a long time. I had the good fortune to be working for the Army CB defense R&D office at Edgewood, Maryland, at the initiation of the CBDP in 1994. Prior to 9/11, it was a messy operation, but it was the only game in town for chem-bio defense. We were a small, scrappy community of technical experts trying to make a difference with a tiny budget. I was also there to see the massive management shift in 2001-2002 that made it a much better-executed program. Not to say that there weren’t screw-ups and massively-inflated egos involved, but in essence just the same issues as any other DoD acquisition program.
Over the last twelve years, the CBDP has significantly changed its direction and effectiveness. OSD acquisition leaders have decided that the services aren’t using the program toward what they thought were national priorities. They changed the regulations and made up new deliberative bodies to move funds away from service-defined requirements, and no one has the desire or will to push back. Protecting the armed forces from deliberate threats of biological weapons was once considered pretty serious work. Diverting funds from that mission to a DOE lab that is primarily focused on nuclear weapons design for a fanciful computer project is a sign that they aren’t serious about that issue.